Military Suicides – Some Numbers and Thoughts
The latest data from the MoD, published in 27 March 2025, show that for the 20-year period 2005-2024, 281 suicides occurred among British regular personnel; 259 males and 22 females. In 2024 there were seven coroner confirmed suicides. There were another nine deaths which may result in a suicide verdict once Coroner Inquests are held.
Some studies (BMJ Military Health) suggest that suicide rates in the Armed Forces are lower than in the general population. Of the three services, the rates are markedly higher in the Army.
Given pre-enlistment medical screening, the over-all good health of the military population, duty of care and the tenets of team-bonding, command and leadership, we should expect suicide levels in the Armed Forces to be very low.
In the veteran community, the picture is rather bleaker. According to Office for National Statistics data released 5 April 2024 and based on the Census of 2021, in 2021 in England and Wales, out of 5,175 suicides in those aged 16 or over, 253 were UK Armed Forces veterans. Of those, 237 were male and 16 female. Notably, in the age range 25 to 44 years, male veterans had a higher rate than in the general population. It is also important to note that the MoD observes that tracking veteran status can be problematic, especially if individuals choose not to so identify.
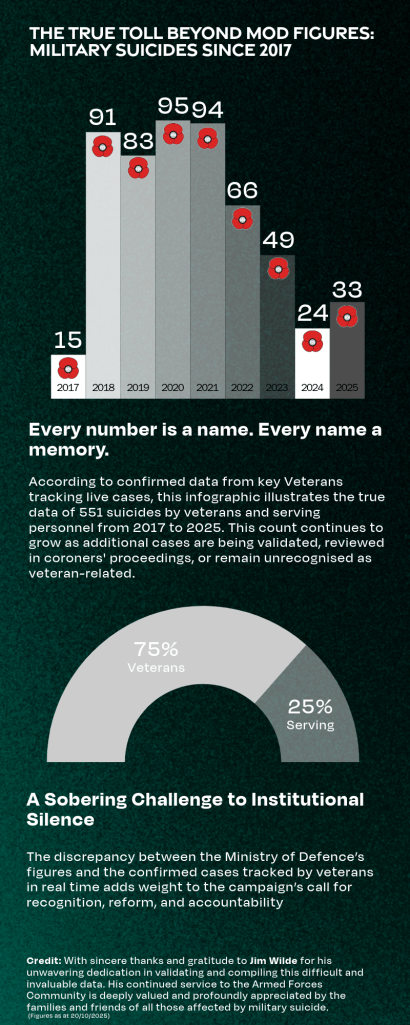
The True Toll Beyond MOD Figures: Military suicides since 2017
By contrast, VUAS’s figures represent confirmed cases within the veteran and military community, often uncovered through grassroots tracking, coroners’ reports, and family engagement. This reveals a troubling gap between official reporting and lived reality.
This infographic stands as a sobering challenge to institutional silence, urging recognition of the true scale of loss, deeper accountability, and urgent reform.
A Crisis Concealed by Numbers
Official tallies tell only part of the story. Coroner verdicts of misadventure, open findings or accidental death often mask intentional self-harm, while reservists and veterans are routinely omitted from service-era counts. Behind each recorded loss lies an iceberg of unspoken attempts and hidden crises that demands our urgent attention. We also know that, for reasons that remain unexplained, some coroners in England and Wales have chosen not to consider the implication of Lariam in veteran suicides even when compelling evidence has been presented to them.
Beyond Mental-Health Screening
Psychological assessments alone cannot uncover every service member at risk. Traumatic brain injury sustained in training or combat, and the neurotoxic aftermath of anti-malarial drugs such as mefloquine (Lariam), can mirror symptoms of depression, anxiety and substance misuse. Without systematic neurological evaluation and drug-effect screening, these injuries go unrecognised and untreated, skewing both care and research.
The Pharmacological Paradox
Antidepressants such as SSRIs are dispensed routinely by military psychiatry, yet paradoxically they can induce the very symptoms they are meant to treat. Early SSRI use is linked to akathisia, emotional blunting and even heightened suicidal ideation. If the psychiatric community must openly acknowledge these iatrogenic harms, it is inconceivable that the toxic neuropsychiatric effects of Lariam should continue to be so stubbornly denied by official channels.
The Danger of Narrow Agendas
An overemphasis on childhood adversity or substance misuse diverts focus from combat trauma, blast-induced brain injury and medication side-effects. Such tunnel vision not only distorts clinical data but also risks unjustly denying service members war-pension and Armed Forces Compensation Scheme entitlements. Effective policy must resist these reductive lenses.
Towards Holistic Prevention
Every routine check, from enlistment through transition back to civilian life, should integrate mental-health, neurotrauma and Lariam-related assessments, alongside careful monitoring of psychotropic prescriptions. Independent panels must reclassify equivocal deaths and widen definitions to encompass attempts and suicide ideation among serving and former personnel. Leadership training and peer-led outreach will destigmatise neurological referrals and ensure no cry for help goes unheard.
A Collective Responsibility
Each mile walked in memory aims to catalyse transparent oversight, sustained investment and systemic reform. By confronting every hidden layer brain injury, drug effects, misclassification and policy blind spots, we not only honour those we have lost but also safeguard those still in crisis. It is our duty to turn remembrance into prevention and healing.